


Reforming Global Health Architecture Amidst Eroding Multilateralism
By Daniele Fattibene, Tom Hart, Karim Karaki and Marianna Lunardini
The global health landscape is navigating a quiet but profound crisis. After years of pandemic-driven surges in funding, the international community has entered a stark “post-aid” reality marked by severe donor fatigue, shrinking multilateral budgets, and growing geopolitical fragmentation. With the dismantling of USAID and Washington’s withdrawal from the World Health Organization, Governments, multilaterals, NGOs, and implementing partners are facing a fundamental question: how can we boost and reform the global health architecture with crunching public resources?
Recently, the European Think Tanks Group (ETTG) convened an internal webinar bringing together experts from the European Centre for Development Policy Management (ECDPM), the Istituto Affari Internazionali (IAI) and ODI Global. The discussion provided a sobering mapping of the current global health financing landscape, alongside an analysis of how both African States and European capitals are shifting their strategies in response.
The Numbers Behind the Crunch: Material Shortfalls and Stagnant Budgets
The most immediate pressure on global health comes from the pocketbooks of traditional donors and a study warned that, if these trends continue, there could be more than 22 million preventable deaths by 2030. The past year has seen unprecedented shortfalls in recent replenishment rounds for the world’s major global health institutions. On the one hand, pledges for the Global Vaccine Alliance (GAVI) fell roughly 20% short of their target, with decline being only partially mitigated by carrying over unspent funds from the COVID-19 response. On the other hand, pledges for the Global Fund to Fight AIDS, Tuberculosis and Malaria plummeted by 30% short of the target, resulting in a 20% resource reduction compared to the last cycle. Crucially, these figures are in nominal terms. When adjusted for global inflation, the real-term purchasing power of these institutions has contracted even more sharply.
Figure 1: Global Fund and GAVI replenishments did not reach targets and are lower than previous replenishments
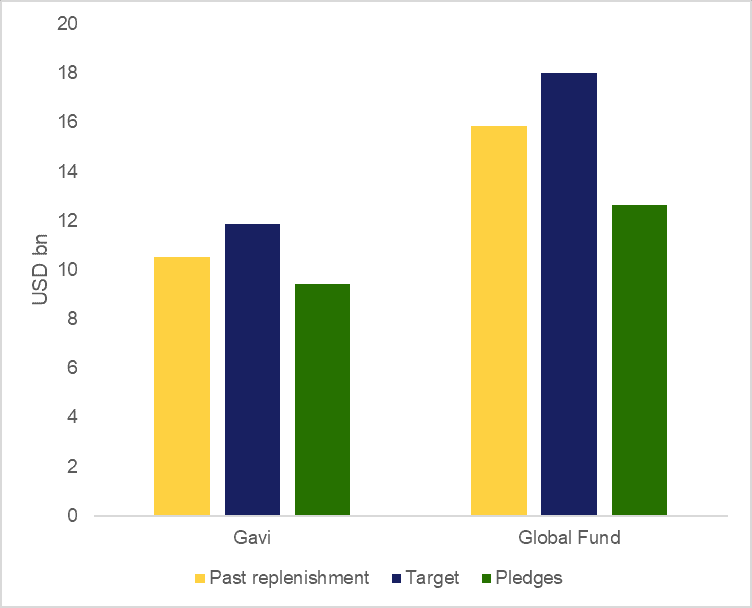
Note: Gavi 5.0 2021-25 is compared to Gavi 6.0 Target & Pledges. Global Fund 7th replenishment 2023-25 is compared to 8th Replenishment 2026-28.
Source for Gavi past replenishment and replenishment target is Protecting Our Future, Investment Opportunity 2026-2030, and Gavi pledging table. Source for Global Fund is the Data Explorer. Figures were correct as of 19th May 2026.
Compounding this multilateral retreat, internal economic pressures are hitting vulnerable nations simultaneously. World Bank projections reveal that government health spending per capita is expected to stagnate or contract in roughly one-third of all low and lower-middle-income countries. In 2024, combined government and donor spending on health averaged just $17 per capita in low-income countries: less than one-third of the $60 estimated minimum needed to deliver a basic package of essential services. In lower-middle income countries, that figure was $47, barely half the benchmark of $90. In highly donor-dependent sectors like health, this double blow – fewer external grants and tighter domestic budgets—threatens decades of progress in primary healthcare.
Figure 2. Annual per Capita Government and Donor Funding Compared to Minimum Benchmark Cost for UHC, 2018 and 2024, LIC and LMIC Median (in Constant 2024 US$)
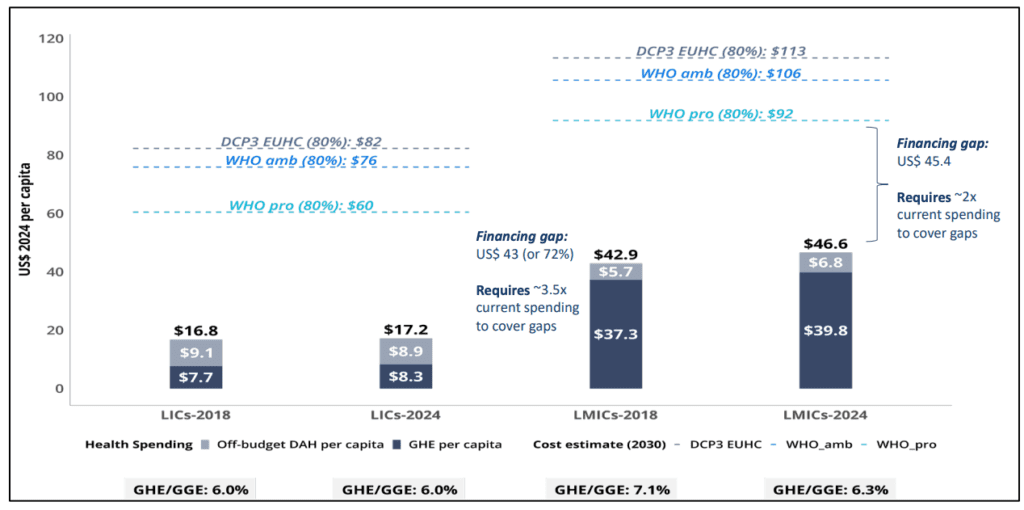
Source: World Bank (2025)
The African Response: Pushing for Health Sovereignty
Faced with a retreating donor landscape, African nations are moving away from the traditional, incremental “aid effectiveness” paradigm. Instead, a more assertive rhetoric centered on global health sovereignty and self-reliance is taking root. This movement is prominently championed by the “Accra Reset” initiative and the Africa CDC’s Health Security and Sovereignty Agenda. These frameworks echo the foundational principles of the Lusaka Agenda (launched in December 2023), which calls for an end to fragmented donor approaches in favor of country-owned primary healthcare system funding. This shift is translating directly into two structural trends. On the one hand, several African countries are accelerating domestic financing, moving with speed to fill budget gaps caused by donor cuts. To provide a few examples of this new African leadership, Nigeria and Ghana boosted their domestic health budgets by approximately $200 million and $300 million respectively, whereas Ethiopia introduced a dedicated payroll tax specifically designed to replace expiring USAID-funded health projects to support its National Health Insurance Scheme. On the other hand, African countries are putting industrial policy and local manufacturing at the core of their policy agendas. Currently, more than 70% of the pharmaceuticals consumed in Africa are imported, mainly from Asia, with local production being heavily concentrated – as eight countries account for 85% of the continent’s approximately 690 pharmaceutical plants. For this reason, during the 39th Ordinary Session of the Assembly of the African Union, African leaders reaffirmed “the continental ambition to meet at least 60 percent of Africa’s health product needs through local manufacturing by 2040”. This aligns with European-supported channels like the African Union–European Union (AU-EU) health partnership and the Team Europe MAV+ vaccine manufacturing initiative in West and East Africa.
Shifting Modalities: How European Capitals are Investing
As the structural dynamics of aid change, European donors are reforming their own toolkits to support global health initiatives, although not in a coordinated manner. The Table below seeks to show how European capitals are prioritizing wildly divergent approaches to navigate this landscape.
Table 1: Global health priorities in a selection of European countries
| Country / Region | Primary Global Health Priorities | Core Financing & Operational Modalities |
| Belgium | Health manufacturing, vaccines, and pharmaceutical sector engagement, Universal Health Coverage & health systems, pandemic preparedness | Strong emphasis on private sector integration utilizing domestic pharma networks; active in Team Europe Initiatives. |
| Germany | Pandemic preparedness and one health | Reduce bilateral health cooperation and funding (except e.g. private coop)and strengthen/ uphold multilateral cooperation and funding, e.g. GAVI |
| Italy | Communicable/non-communicable diseases, universal health coverage, digital health pilots, maternal and child mortality, workforce training. | Multilateral commitments (e.g. GAVI, Global Fund, CEPI) mixed with bilateral alignment under the Piano Mattei; focus on CSO partnerships (e.g., CUAM, Sant’Egidio) and private-sector triangulation. |
| Luxembourg | Traditional primary/maternal healthcare services, universal health coverage, SRHR etc. | Direct sovereign finance channeled via traditional government sector budget support. |
| Spain | Health system strengthening, governance, innovation/research, maternal and child health, multilateral engagement rooted in One Health and human rights frameworks. | Joint governance via Foreign Affairs and Health ministries under the Spanish Global Health Strategy 2025–2030; constrained by domestic budget uncertainties. |
| The Netherlands | Sustainable health financing and Sexual and Reproductive Health and Rights (SRHR), global health architecture and national health systems, One Health, pandemic preparedness etc. | Developing innovative financing mechanisms with civil society to move away from pure grant dependency. |
| United Kingdom | Global health security, strengthening country health systems and reforming the global health architecture. | Supporting global health especially via multilateral funds (e.g. The UK is the largest donor of GAVI and the 3rd largest donor of the Global Fund to Fight AIDS, Tuberculosis and Malaria) |
Some of the main bottlenecks to address
A common thread across many European strategies – and explicitly highlighted in the UK’s post-aid-cut rhetoric—is a desire to move from being a “donor” to an “investor”. However, translating this corporate enthusiasm into actual health outcomes is proving incredibly difficult. Private companies face steep entry barriers in global health deployment, driven by high perceived risks, a lack of clear market data, and limited baseline familiarity with African healthcare markets. In addition, there are still doubts on the role and responsibilities of Public Development Banks and Development Finance Institutions in health (given the reliance of health systems on public funding, often in the form of grants), thus on the resources they could unlock to address global health priorities.
In addition to the financing stalemate, there are emerging frictions that threaten to stall modern health interventions, particularly in the digital and artificial intelligence (AI) space. While digital health pilots and telemedicine show immense promise, severe data-sharing frictions and geopolitical tensions around data sovereignty have recently stalled critical US bilateral agreements in countries like Nigeria, Zambia and Ghana. Navigating data privacy, intellectual property, and local infrastructure capacity remains a complex regulatory hurdle for donors attempting to introduce high-tech health solutions.
Furthermore, there appears to be a distinct lack of global leadership willing to champion deep structural architecture reforms. For instance, at the World Health Assembly in Geneva, draft frameworks reviewing the global health architecture explicitly barred the process from proposing fundamental changes to organizational mandates or consolidations. This gridlock leaves middle powers—predominantly European countries —with the responsibility to step into this leadership vacuum.
Moving Forward: Key Upcoming Milestone Events
As the global health community works to reconcile shrinking funding envelopes with rising localized demands, the upcoming months feature several key milestones where these debates will play out in practice. The next G20 UK Presidency offers a great chance to bring global health at the top of leaders policy agendas. Though the UK is expected to prioritize broad finance-track themes like Multilateral Development Bank (MDB) reform, private finance mobilization, and debt relief rather than standalone global health architecture reform, experts are watching closely to see if London will resurrect the G20 highly influential joint Health-and-Finance Task Force, established under the Italian G20 Presidency in 2021.
Ultimately, the ETTG webinar underscored a profound truth: the era of unstructured, grant-heavy external health aid is winding down. The future of global health survival will rely on how effectively the international architecture can pivot toward true national sovereignty, robust local pharmaceutical manufacturing, and coordinated, innovative financing mechanisms.

